Figure 2: Intraoperative photograph demonstrating dry cancellous bone surfaces of the distal femur and proximal tibia, ideal for cement interdigitation.
Courtesy of Paul Issack, MD
Published 1/29/2026
The use of a tourniquet during primary cemented total knee arthroplasty (TKA), while once a near-universal practice, has recently come into question. Literature suggests that outcomes after total knee replacement are similar regardless of whether a tourniquet is used. Thus, whether to use a tourniquet during TKA has become a matter of surgeon preference.
The following article highlights four surgeons and three perspectives on tourniquet use, including no tourniquet, full tourniquet (in use throughout the case), and limited tourniquet (inflated during cementing).
The surgeons include:
- Michael DeRogatis, MD, MS, is an orthopaedic surgery resident at St. Luke’s University Health Network in Bethlehem, Pennsylvania.
- Mark L. Brandon, MD, FAAOS, is an adult reconstruction orthopaedic surgeon at Richmond University Medical Center, Staten Island, New York.
- Markku Nousiainen, MS, MEd, MD, FRCSC, FAAOS, FAOA, is an associate professor of surgery at the University of Toronto and a lower extremity reconstruction and trauma surgeon at Sunnybrook Health Sciences Centre in Toronto, Ontario, Canada.
- Paul S. Issack, MD, PhD, FAAOS, FACS, is a clinical associate professor in the Department of Orthopaedic Surgery, Weill Cornell Medical College, and a trauma and adult reconstruction orthopaedic surgeon at New York-Presbyterian/Lower Manhattan Hospital and Richmond University Medical Center in Staten Island, New York. He is also a member of the AAOS Now Editorial Board.

Figure 1: Intraoperative photograph demonstrating Esmarch bandage application prior to tourniquet inflation just before cementing in primary total knee arthroplasty.
Courtesy of Paul Issack, MD
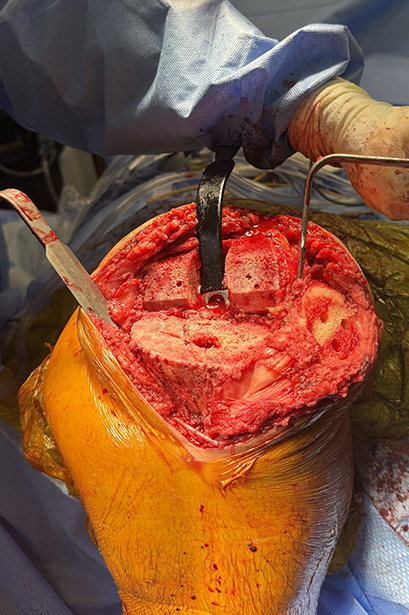
Figure 2: Intraoperative photograph demonstrating dry cancellous bone surfaces of the distal femur and proximal tibia, ideal for cement interdigitation.
Courtesy of Paul Issack, MD
Dr. DeRogatis – No tourniquet
Although tourniquets have long been a fixture in primary TKA, contemporary data make their routine use increasingly difficult to justify. Tourniquet inflation induces immediate muscle ischemia and neural compression, resulting in measurable clinical deficits during the early recovery period.
At two weeks after TKA using a tourniquet, patients consistently report higher pain scores and reduced knee range of motion compared with tourniquet-free surgery. By four weeks, this disadvantage persists, with greater thigh and knee swelling and slower normalization of gait and functional use of the limb, as found in a study by Wang et al.
These effects extend well beyond the first month. Alexandersson et al. found that, at three months, patients demonstrate a slower Timed Up and Go test despite otherwise uncomplicated surgeries. Such patterns are even more concerning in individuals with relative contraindications, including peripheral arterial disease, prior vascular bypass, popliteal aneurysm, clotting disorders, fragile skin, or patellar maltracking, where the risk-benefit balance tilts even further against tourniquet use, shown by research from Cho et al., Komatsu et al., and Turner et al.
Complications such as peroneal nerve injury, vascular compromise, and anesthesia-related tourniquet pain occur after about one hour, marked by hypertension and tachycardia (see research by Nercessian et al. and Troutman et al.). Moreover, the supposed advantages of tourniquets have diminished. According to research from Ozkunt et al., excellent visualization is achievable once the knee is flexed, and modern hemostatic practices, including the use of tranexamic acid, produce reliable cement fixation without requiring a bloodless field. When weighed against delayed recovery, physiologic strain, risk of complications, and increased costs, routine tourniquet use offers little value. A tourniquet-free TKA aligns more closely with contemporary goals of enhanced recovery, improved early function, and reduced perioperative risk.
Drs. Brandon and Nousiainen – Full tourniquet
Many surgeons routinely perform primary TKA with a tourniquet inflated before skin incision. The tourniquet is deflated after the cement has hardened to look for bleeding vessels before wound closure. Tourniquet use throughout the case permits clear visualization of the joint, which makes it easier to perform the requisite bone cuts and soft tissue releases.
There is evidence that tourniquet use during cemented primary TKA can reduce the length of surgery, decrease intraoperative blood loss, and improve cement penetration. Zhou and colleagues conducted a prospective, double-blinded, randomized controlled trial, demonstrating shorter surgical times in the tourniquet group. Boutros and colleagues, in a meta-analysis of 50 randomized controlled trials, showed that tourniquet use slightly decreased operative time for cemented TKA. The same study showed a significantly lower intraoperative blood loss with tourniquet use. Johnsen et al. in a randomized trial showed significantly greater intraoperative blood loss in TKA performed without tourniquet. Mirahmadi et al. in a meta-analysis showed that tourniquet use in TKA was associated with a 52% reduction in blood loss and increased cement penetration.
However, we acknowledge that there are specific clinical scenarios which may preclude full tourniquet use. These include patients with vascular conditions including vascular insufficiency, clotting disorders such as sickle cell hemoglobinopathy, prior vascular bypass, popliteal aneurysm, or a history of an extensive DVT in the ipsilateral limb. When a venous tourniquet is in place, it must be deflated to perform the knee replacement and minimize blood loss.
Dr. Issack – Limited tourniquet
For routine total knee replacement, some surgeons prep the leg with a thigh tourniquet but do not inflate it until just before cementing. While tourniquets have been associated with a lower intraoperative blood loss and shorter operative time, there is a substantial risk for postoperative drainage as well as thigh and knee pain. According to research from Boutros et al. and Katzman et al., there have been no significant differences noted between the use of opioids, hemoglobin levels, transfusion requirements, or knee functional scores. A surgeon can achieve a relatively dry field until the bone cuts are performed. Tourniquet is inflated during implant cementing and deflated after the cement has hardened. This approach mitigates the risk of a vascular injury that may not be noted until after the implants are in. In some cases, vasospasm after tourniquet deflation may prevent the detection of a vascular injury for several minutes.
A second reason to avoid inflating a tourniquet for the entire case is that many patients report thigh and knee pain when tourniquets have been in place for more than 60 minutes.
When a case takes longer than expected, the limited tourniquet method removes worry about tourniquet time. Thirdly, the risk of increased bleeding from a venous tourniquet, common in obese patients, is eliminated.
Doing TKA without a tourniquet makes it challenging to obtain a dry, bony cancellous bed, which is required for good cement technique. Only 10-15 minutes of tourniquet time is required for this portion of the operation, a reasonable compromise in avoiding tourniquet-related complications but also allowing for good cement fixation.
In short, brief, targeted tourniquet inflation during cementing provides a practical middle ground that preserves fixation quality while minimizing tourniquet related complications.
Conclusions and confounding factors
Within the tourniquet literature, multiple variables can influence outcomes. Reported blood loss can be subjective and may be influenced by tranexamic acid use, timing of tourniquet deflation, and type of anticoagulant used for deep vein thrombosis (DVT) prophylaxis. Pain scores can be influenced by the use of regional and local anesthetic agents in the perioperative period.
Range of motion can be influenced by the preoperative range of motion, type of prosthesis being inserted, the amount of contour in the polyethylene liner, the amount of constraint in the implant, the amount of soft tissue release being performed, the postoperative rehabilitation protocol, or the severity of the preoperative joint contractures.
Decision-making on tourniquet use often stems from training. As studies emerge that challenge traditional techniques, surgeons should thoughtfully assess the literature and consider adjustments to their practices.
References:
- Wang, K, Ni, S, Li, Z, et al. The effects of tourniquet use in total knee arthroplasty: a randomized, controlled trial. Knee Surg Sports Traumatol Arthrosc. 2017;25:2849-2857. doi:10.1007/s00167-015-3964-2
- Alexandersson, M, Wang, EY, Eriksson, S A small difference in recovery between total knee arthroplasty with and without tourniquet use the first 3 months after surgery: a randomized controlled study. Knee Surg Sports Traumatol Arthrosc. 2019;27:1035-1042. doi:10.1007/s00167-018-5196-8
- Cho, MR, Kim, KT,Choi, WK. (Arterial occlusion after total knee arthroplasty despite minimal invasive technique in aneurysm at popliteal artery: case report. Medicine (Baltimore). 2018;97, e12719. doi10.1097/MD.0000000000012719
- Komatsu T, Ishibashi Y, Otsuka H, Nagao A, Toh S. The effect of surgical approaches and tourniquet application on patellofemoral tracking in total knee arthroplasty. J Arthroplasty. 2003;18:308-312. doi:10.1054/arth.2003.50057
- Turner NS III, Pagnano MW, Sim FH. Total knee arthroplasty after ipsilateral peripheral arterial bypass graft: acute arterial occlusion is a risk with or without tourniquet use. J Arthroplasty. 2001;16:317-321. doi: 10.1054/arth.2001.21502
- Nercessian OA, Ugwonali O F, Park S. Peroneal nerve palsy after total knee arthroplasty. J Arthroplasty. 2005;20:1068-1073. doi:10.1016/j.arth.2005.02.010
- Troutman DA, Dougherty MJ, Spivack AI, Calligaro KD. Updated strategies to treat acute arterial complications associated with total knee and hip arthroplasty. J Vasc Surg. 2013;58:1037-1042. doi:10.1016/j.jvs.2013.04.035
- Ozkunt O, Sariyilmaz K, Gemalmaz HC,Dikici F. The effect of tourniquet usage on cement penetration in total knee arthroplasty: a prospective randomized study of 3 methods. Medicine (Baltimore). 2018;97:e9668. doi:10.1097/MD.0000000000009668
- Zhou K, Ling T, Wang H, et al. (Influence of tourniquet use in primary total knee arthroplasty with drainage: a prospective randomised controlled trial. J Orthop Surg Res. 2017;12:172. doi:10.1186/s13018-017-0683-z
- Harsten A, Bandholm T, Kehlet H, Toksvig-Larsen S. Tourniquet versus no tourniquet on knee-extension strength early after fast-track total knee arthroplasty: a randomized controlled trial. Knee. 2015;22:126-130. doi:10.1016/j.knee.2014.12.010
- Tarwala R, Dorr LD, Gilbert PK, Wan Z, Long WT. Tourniquet use during cementation only during total knee arthroplasty: a randomized trial. Clin Orthop Relat Res. 2014;472:169-174. doi:10.1007/s11999-013-3124-2
- Boutros M, Awad G, Abboud E, Zhao A, S CT. Total knee arthroplasty with or without a tourniquet: a meta-analysis of randomized controlled trials. Eur J Orthop Surg Traumatol. 2025;35:397. doi:10.1007/s00590-025-04492-1
- Katzman JL, Sandoval CG, Roof MA, Rozell JC, Meftah M, Schwarzkopf R. Does the use of a tourniquet influence five-year outcomes following total knee arthroplasty? J Arthroplasty. 2025;40:S208-S213. doi:10.1016/j.arth.2024.11.021
- Johnsen M, Havik, S, Husby VS, Winther SB, Foss OA, Husby OS,Lian OB. The use of tourniquet in total knee arthroplasty does not impact the functional outcome: a randomized controlled study. J Orthop Surg Res. 2024;19:704. doi:10.1186/s13018-024-05203-y.
- Mirahmadi A, Parvandi A, Mohammaditabar M, Eidgahi DR, Dorabad AS, Amiri S, Tayyebi H, Li M, Nazarian A. Tourniquet effect on cement penetration in total knee arthroplasty: a systematic review and meta‐analysis. J Exp Orthop. 2025;12:e70380. doi:10.1002/jeo2.7038